
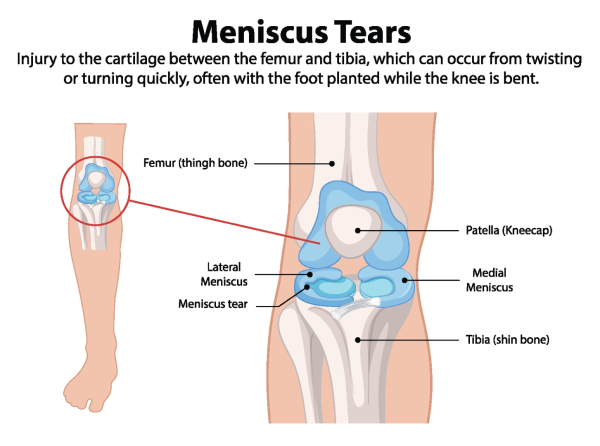
The menisci are wedge-shaped pieces of fibrocartilage that sit between your femur (thigh bone) and tibia, acting as shock absorbers during weight-bearing movement. The two menisci in each knee, the medial meniscus on the inner side and the lateral meniscus on the outer side, help distribute weight, protect cartilage, and stabilize the knee joint during daily activities and sports.
Here’s the surprising truth: not every meniscal tear causes severe knee pain. Some tears produce only vague aching, while others remain completely painless. In fact, studies show that over one-third of adults over 50, and up to 60% of those over 70, have degenerative meniscus tears visible on MRI without any symptoms. Many Buford, GA residents in their 40s–70s discover tears incidentally when imaging is ordered for general knee stiffness.
This raises an important question: if a tear doesn’t hurt, does it matter? The answer is yes. Even minimally symptomatic tears can progress, damage cartilage, and accelerate osteoarthritis. Early evaluation, before a tear worsens, protects your long-term knee health.
At Academy Orthopedics, our orthopedic specialists in Buford, GA, have the expertise to evaluate your knee, interpret your imaging accurately, and recommend the right course of action for your specific situation, whether that is active monitoring or a targeted surgical solution. Early evaluation is the single most effective step you can take to protect your knee health for the long term. Schedule your consultation with Academy Orthopedics today at 770-271-9857 and get a clear, honest answer about what your knee needs.
What Types of Meniscus Tears May Be Painless?
Symptom intensity of meniscal tear depends heavily on tear pattern, location within the meniscus, and blood supply, each factor influencing whether a tear stays quiet or becomes painful.
Inner-zone (white-zone) tears sit in the avascular area of the meniscus, where limited blood supply and fewer nerve endings mean these tears may cause only vague aching or no pain at all.
Degenerative tears develop gradually in adults over 45-50 due to age-related tissue breakdown, with or without accompanying arthritis. These tear patterns often appear on MRI even when the main complaint is stiffness rather than sharp pain.
Chronic, stable tears occur when the knee has adapted over months or years. Patients may notice fatigue, mild swelling after walking around Lake Lanier, or difficulty with deep squats, but no acute injury or sudden pain.
Flap and intrasubstance tears each present differently. Flap tears have a displaced segment that intermittently folds into the joint space, causing occasional catching or brief twinges. Intrasubstance tears remain contained within the meniscal tissue and often produce no mechanical symptoms at all.
What Factors Influence How Much a Torn Meniscus Hurts?
Two people with similar MRI findings can experience vastly different pain levels. Several factors explain this variation:
| Factor | Higher Pain | Lower Pain |
|---|---|---|
| Tear location | Outer “red zone” with blood vessels and nerves | Inner “white zone” with limited blood supply and fewer nerve endings |
| Onset/mechanism | Traumatic meniscal tear in young athlete | Degenerative tear developing gradually |
| Knee health | Concurrent ACL injury or arthritis | Isolated tear in healthy joint |
| Activity level | Construction worker climbing ladders | Office worker with sedentary routine |
Overall, traumatic tears from a specific injury often produce immediate, sharp knee pain, while degenerative changes creep up gradually with softer symptoms.
👉Also Read: What are Meniscal Tears, and How do Orthopedic Surgeons Help Fix Them?
What Are the Subtle Signs You Might Have a Torn Meniscus Even If the Pain Is Mild?

Many Buford patients are surprised to learn their meniscus is torn because they never had a dramatic sports injury or felt a popping sensation.
Watch for these subtle signs:
- Intermittent catching or clicking when standing from a chair or using stairs
- Mild swelling appearing later in the day or the morning after hiking at Buford Dam Park
- A sense of vague instability or subtle hesitation when pivoting or changing direction, even without sharp pain
- Difficulty fully bending or straightening the knee in certain positions, such as kneeling to garden or lying in a bent position
These mechanical symptoms often indicate the meniscus is being intermittently impinged or displaced within the joint, even when pain remains minimal.
What Are the Common Myths About Meniscus Tears?
Misunderstandings delay medial meniscus tear treatment and lead patients to ignore early warning signs.
Myth 1: Every torn meniscus is excruciating.
Reality: Most meniscus tears cause mild aching or stiffness. Inner-zone tears may produce no pain at all, yet still damage cartilage over time.
Myth 2: Only athletes tear their meniscus.
Reality: This common knee injury happens to Buford residents stepping off curbs, rising from low chairs, or moving into a squatting position, especially after age 40.
Myth 3: Surgery is always required.
Reality: Research shows many degenerative tears without locking respond well to conservative treatment. The ESCAPE trial found that exercise therapy was noninferior to arthroscopic partial meniscectomy at two years for patients with degenerative meniscal tears without mechanical locking.
Myth 4: Painless tears cannot get worse.
Reality: Tears can enlarge and accelerate cartilage wear, raising osteoarthritis risk even without symptoms.
Myth 5: Rest alone heals any tear.
Reality: Because the inner two-thirds of the meniscus has poor blood supply, rest may reduce inflammation, but cannot structurally repair most tears. Outer-zone tears in younger patients have greater healing potential, but still require proper assessment.
Myth 6: Knee locking always means a meniscus tear.
Reality: True mechanical locking is most often associated with bucket-handle meniscal tears, but loose cartilage fragments, bone spurs (osteophytes), or pain-inhibited motion from arthritis can produce similar-feeling symptoms. An orthopedic evaluation can distinguish between the two.
Myth 7: Meniscus issues only matter for young people.
Reality: Protecting the meniscus helps adults in their 50s, 60s, and beyond avoid early knee replacement.
👉Also Read: Easily Identify the Symptoms of a Meniscus Tear in 5 Easy Steps
When a Meniscus Tear Can Progress Without Much Pain
Absence of severe pain does not guarantee safety from long-term damage.
A small tear can gradually extend within the meniscal tissue over months of normal weight-bearing activity, changing in size, pattern, or depth. This progressive damage increases cartilage wear on the femur and tibia, leading to joint space narrowing visible on X-ray. Subtle instability or altered gait from guarding the injured knee can also strain surrounding ligaments and increase load on the opposite compartment of the same knee or the contralateral limb.
For active patients or those whose jobs require frequent kneeling or lifting, periodic monitoring with clinical exams and possibly repeat imaging helps catch progression early.
How Orthopedic Specialists Diagnose “Silent” or Minimally Painful Meniscus Tears in Buford, GA
A typical first visit involves reviewing your symptom history, activity level, and goals, followed by a thorough physical exam.
Physical exam maneuvers include:
- McMurray test (applying rotational stress while moving the knee from full flexion toward extension to detect a click or joint line pain)
- Thessaly test (weight-bearing rotation with the knee held at 20 degrees of flexion)
- Joint line tenderness palpation
These detect mechanical symptoms even when pain is mild.
X-rays assess for arthritis, alignment issues, and bone problems that can mimic or accompany meniscus injury.
MRI is ordered when symptoms persist, catching, swelling, or instability, when conservative treatment has not provided adequate relief, or when planning surgical treatment for athletes and active adults. It also helps identify concurrent ligament or cartilage injuries that may not be apparent on examination alone. A sports medicine or orthopedic specialist familiar with both traumatic and degenerative patterns helps distinguish clinically important findings from incidental wear.
What Are the Treatment Options for Minimally Symptomatic Meniscus Tears?
Treatment in Buford is highly individualized based on symptoms, tear pattern, age, arthritis level, and patient goals.
Conservative management
- Activity modification (avoiding deep squats, twisting, and high-impact sports)
- Short-term anti-inflammatory medications or acetaminophen
- Compression, elevation, and supportive or unloader bracing to reduce swelling and offload the affected compartment
Physical therapy
A physical therapist designs programs to strengthen the muscles around the knee, quadriceps, hamstrings, hip, and core to decrease swelling, improve knee motion, and offload the meniscus.
Injections
- Corticosteroids relieve pain and reduce inflammation for moderate symptoms
- Hyaluronic acid injections are sometimes used for arthritic knees, though evidence of benefit remains mixed and is best discussed with your orthopedic specialist
- Platelet-rich plasma (PRP) is an emerging option being used in some cases to support tissue healing, though research on its effectiveness for meniscal tears is still evolving
Surgical options
Arthroscopic surgery may be recommended when the knee locks, motion is significantly restricted, or when an adequate trial of nonsurgical treatment, typically 6–12 weeks for degenerative tears, has not provided sufficient relief. Acute traumatic tears with true mechanical locking may require earlier surgical evaluation. Surgeons use a tiny camera and minimally invasive technique to perform partial meniscectomy (trimming the torn fragment) or meniscal repair (suturing the meniscus when blood supply and tear pattern allow).
What Are the Emerging and Advanced Therapies for Meniscus Preservation?
Latest torn meniscus treatments aim to protect the meniscus and slow arthritis progression.
Platelet-rich plasma (PRP): Emerging research suggests PRP injections may reduce pain and improve function in some patients with degenerative tears, though results vary depending on injection technique, tear pattern, and follow-up length. One study of 392 patients with degenerative tears found that 90% avoided surgery at 18-month follow-up, with significant short-term improvements in pain and function. However, longer-term comparative studies show more variable results, and PRP is best considered a promising emerging option rather than a proven standard of care. PRP does not regrow lost tissue.
Stem cell therapies: Research continues on cell-enhanced scaffolds and regenerative approaches, though these remain evolving rather than standard care.
Advanced arthroscopy: Modern techniques, including all-inside, inside-out, and outside-in meniscal repair methods, preserve as much tissue as possible, with technique selection based on tear location and pattern.
Structured rehabilitation: After biologic or surgical treatment, a phased rehabilitation plan progresses from walking to low-impact exercise to higher-demand sports as strength returns.
👉Also Read: Meniscus Tears: The Importance of Treating Them Without Delay
Get an Expert Knee Evaluation at Academy Orthopedics in Buford, GA
If you have noticed catching, mild swelling, stiffness, or hesitation when pivoting, your knee is telling you something worth listening to. A meniscal tear does not have to be painful to deserve attention, and waiting until pain becomes severe often means managing a larger problem later.
At Academy Orthopedics, our board-certified orthopedic physicians, including Dr. Jesse E. Seidman, Dr. James W. Duckett III, and Dr. Jonathan Katz, bring Fellowship-trained expertise across knee surgery, sports medicine, and arthroscopic procedures. Whether your concern is a degenerative tear discovered on imaging or a mechanical symptom that has been quietly limiting your daily life, our team evaluates each patient individually, without defaulting to surgery when conservative care is the right first step.
Our on-site ambulatory surgical center means that if treatment does progress to a procedure, you benefit from a streamlined, convenient experience without hospital-based delays.
Serving Buford and the surrounding communities of Cumming and Duluth, Academy Orthopedics is equipped to manage both traumatic and degenerative meniscal conditions from first evaluation through full rehabilitation.
Do not wait for a quiet tear to become a louder problem. Call us at (770) 271-9857 or schedule your appointment online to protect your knee health today.
Frequently Asked Questions
Can I keep working or exercising if my torn meniscus does not hurt much?
Many patients can continue working and doing low-impact exercise with a small or minimally symptomatic tear. However, avoid high-impact activities, twisting, and deep squatting until an orthopedic specialist evaluates which activities are safe for your specific injury.
How long can I safely wait before seeing a doctor for a suspected meniscus tear?
Seek evaluation within a few weeks if meniscus tear symptoms like swelling, catching, or stiffness persist, even without severe pain. If the knee locks, suddenly cannot fully straighten when it could before, or becomes acutely unstable, schedule a same-week appointment.
Is an MRI always necessary to diagnose a torn meniscus?
Not always. Many tears can be strongly suspected based on history and physical exam. MRI is particularly helpful when symptoms are subtle, the diagnosis is uncertain, or when planning for meniscus surgery or advanced therapies.
Will a knee brace help if my torn meniscus does not hurt but feels unstable?
A supportive or unloader brace can help reduce instability and offload the affected compartment, particularly when arthritis accompanies the tear. However, bracing does not heal the tear itself and should be combined with strengthening exercises and medical guidance.
What signs mean my meniscus tear is getting worse?
Warning signs include increasing pain with daily activities, more frequent swelling, new or more severe locking episodes, and reduced ability to fully bend or straighten the knee. Any of these changes should prompt a follow-up visit for reassessment and possible updated treatment options.